

Which infectious ailment ranks as the most lethal globally? HIV? COVID-19? Malaria?
The response is tuberculosis. This disease claims over 3,400 lives worldwide every day — nearly 1.3 million in 2023 alone — and that figure is rapidly escalating. Without intervention, tuberculosis (TB) can literally suffocate you. Or it may spread to your brain, lymph nodes, bones, or kidneys — anywhere that your bloodstream can transport it.
In the United States, we view TB as a remnant of earlier times, a romantically tragic affliction where frail, flushed young women with bright eyes (due to fever, mind you) coughed up blood into lace handkerchiefs, bid soft farewells, and passed away. But TB has been eradicated, hasn’t it?
[TB] instances across the nation (though still minimal compared to the rest of the world) are increasing by around 7% annually — with limited public awareness of this resurgence.
TB did see stricter management in the U.S. during the 1950s, thanks to public health initiatives and the discovery of the antibiotic streptomycin. However, in the 1980s, public health reductions under Reagan and the AIDS crisis reversed that progress. Yet, by 1993, cases were again decreasing steadily, by roughly 7% each year. This trend continued until 2020, when the COVID-19 outbreak artificially depressed the rate further since diagnoses plummeted. However, the delay in prompt treatment allowed TB to regain traction. Currently, instances nationwide (still minor compared to the global situation) are also rising by about 7% each year — with scant public knowledge of the resurgence.
This could evolve with a new WashU initiative — the Mycobacteria-centered Program for Research and Innovation in Science and Medicine (MycoPRISM) — that is uniting specialists from various fields. They will analyze TB’s origins and explore new therapies from multiple perspectives. In tandem, the recently established School of Public Health, the university’s first new establishment in a century, will work towards enhancing awareness and education, eliminating stigma, and tackling root causes.
Worldwide, 2023 saw a record surge in new diagnoses — approximately 8.2 million, the highest tally since the World Health Organization started tracking 30 years ago, according to the Journal of the American Medical Association (January 2025). More than a quarter of all humans currently alive have already been infected. Often, Mycobacterium tuberculosis remains latent, but any weakening of the immune system can activate it, even 80 years after the initial infection. Furthermore, just one person with infectious TB can transmit the illness. Across borders.
Reasons this challenge is difficult to address
When paleogeneticists examined ancient mummies, they uncovered them filled not with human DNA, which had deteriorated, but with tuberculosis DNA. TB is the disease that has proven enduring.
“TB has been infecting and causing fatalities among humans for eons,” states Christina Stallings, PhD, a WashU Medicine professor of molecular microbiology and the Theodore and Bertha Bryan Professor of Environmental Medicine. “Yet, we still have not managed to control it. Why is that?”
Because it is ancient and has evolved alongside us. It has had millennia to hone its ability to manipulate our immune systems. It’s transmitted through the air via the incessant coughs of infected individuals. Still, in a laboratory setting, it proliferates at an agonizingly sluggish pace, complicating research efforts. Furthermore, we lack an effective vaccine to shield adults from the disease.
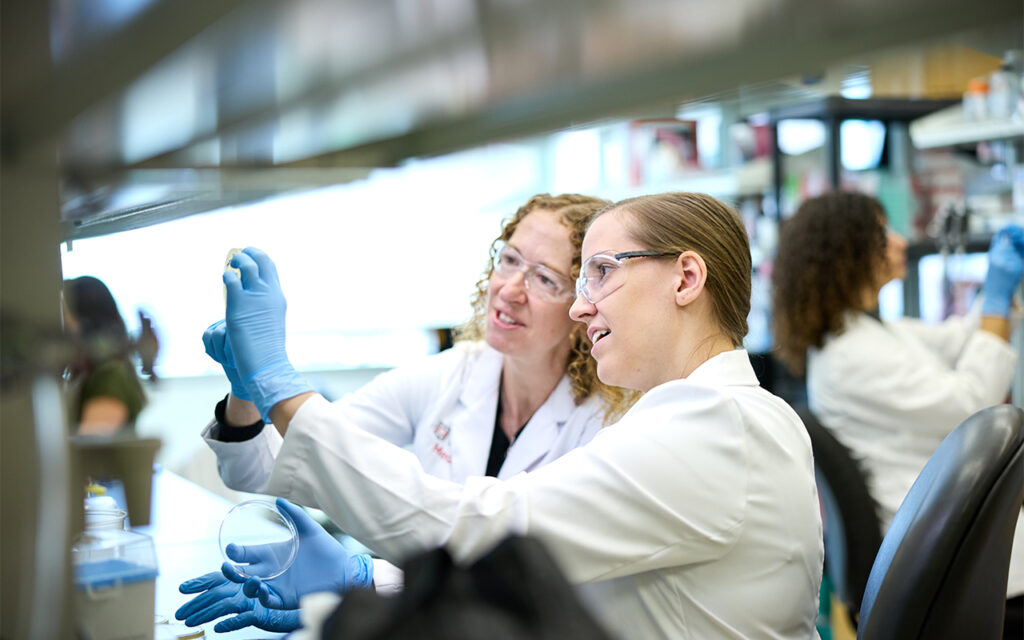 Christina Stallings, PhD (left) collaborates with postdoctoral research associate Abigail Garrett, PhD. In the Stallings lab, researchers investigate how M. tuberculosis defends itself against the immune system and withstands antibiotic treatment. (Photo: Matt Miller/WashU Medicine)
Christina Stallings, PhD (left) collaborates with postdoctoral research associate Abigail Garrett, PhD. In the Stallings lab, researchers investigate how M. tuberculosis defends itself against the immune system and withstands antibiotic treatment. (Photo: Matt Miller/WashU Medicine)In adults, TB typically hides within the lungs, where it can evade the immune system. In children, whose immune defenses are less robust, it spreads to other areas of the body. Fortunately, a vaccine exists to shield children against severe consequences. However, once again, there is no effective vaccine available to protect adults from TB.
Due to M. tuberculosis’s exceptional ability to safeguard itself, standard treatment may require a full six months or more. A combination of four different drugs is utilized, designed to thwart the bacteria from developing resistance. However, these antibiotics can make some individuals unwell, causing them to discontinue treatment. Others may feel better quite rapidly, leading them to stop their medication.
“TB has been infecting and causing fatalities among humans for eons. Yet, we still have not managed to control it. Why is that?”
Christina Stallings, PhD
Still present in the body, the bacteria may cause a patient’s condition to deteriorate or lead to a relapse. And if the medications are not properly prescribed or taken, the bacteria will develop resistance to them, rendering TB even more challenging to manage.
Even if a patient completes the full treatment course and shows improvement, the bacteria might simply find a quiet area to enter dormancy. “We have no means to determine who truly eradicates it,” Stallings clarifies. “Thus, it becomes extremely difficult to fight this pathogen when we can’t even identify who is infected!”
In her laboratory, Stallings explores how M. tuberculosis defends itself against the immune system and survives antibiotic treatment. What sets mycobacteria apart, a subset of microbacteria, is that they are enveloped in a casing finely coated by fatty mycolic acids. This covering serves as both a disguise and armor: It can actually deceive the immune system into assisting a pathogen it should have eliminated on sight. Should that fail, TB has developed alternate strategies to endure an assault.
Enter the mice.
TB can infect any warm-blooded animal — two elephants at the Saint Louis Zoo, for instance, have been diagnosed in the past 15 years. “They’re healthy; they were very effective at adhering to their antibiotic regimen,” Stallings notes. “But it’s the mice from whom we’ve gained significant insights.”
“We possess this crucial immune cell in our bodies called a neutrophil … And what we discovered is that the neutrophils, instead of eliminating the bacteria, are actually enhancing their ability to induce disease.”
Christina Stallings
“We possess this crucial immune cell in our bodies known as a neutrophil,” she explains. “Our bloodstream is teeming with them, and they attack and consume anything that attempts to invade us. When we examined the lungs of TB patients, we found numerous neutrophils attempting to eliminate the TB — yet, the individuals remained unwell. We observed a similar phenomenon in our mice. And what we discerned is that the neutrophils, rather than destroying the bacteria, are actually enhancing their capacity to induce disease.”
A neutrophil has an array of weapons, one of which is an extracellular trap. “Envision a delightful round cell ejecting a web akin to a spider’s, laden with deadly substances,” Stallings elaborates. “That web is intended to ensnare whatever it seeks to neutralize — yet mycobacterial TB has discovered a way to thrive on those lethal components.
“`html
nets. It has a fondness for them. Therefore, we’ve succeeded in obstructing the neutrophil’s capability to generate that net.” Fortunately, medications were already being designed to achieve that, since the nets also present issues for arthritis and autoimmune ailments. “We aspire to utilize the same medications to address TB.”
However, she cannot take a moment to relish that achievement; considerably more must be uncovered. In the meantime, a novel challenge is surfacing: Other mycobacteria, which exist naturally in soil and water, are instigating illnesses that are even more challenging to manage. “They have developed the capability to induce lung infections in individuals with diminished lung functionality or those who are immunocompromised,” she clarifies. “They typically cause infections only when an underlying condition is present, but when they do, treatment becomes significantly more complicated.”
Mycobacterium abscessus is among them, and undoubtedly the most severe. The individuals most impacted are those with cystic fibrosis, for whom treatment of the infection is sometimes impossible. Stallings inhales deeply. “It’s dreadful. And the occurrence of these bacteria is on the rise.”
Why at this moment? “It’s not entirely understood,” she explains. “However, Fangqiong Ling (an assistant professor in energy, environmental and chemical engineering at the McKelvey School of Engineering) is investigating the environmental reservoirs,” locations of water or soil where they flourish.
This type of cooperation will be increasingly common, thanks to the MycoPRISM initiative. As co-director, Stallings is gathering specialists: “Numerous individuals at WashU are keen on mycobacteria — clinicians, fundamental science researchers, chemists, engineers, public health specialists — yet we have all been working independently in separate silos.” By sharing insights, we can construct a premier hub of knowledge.
Transforming the landscape of the epidemic
The initiative’s other co-director is Jennifer Philips, MD, PhD, a professor of medicine and molecular microbiology at WashU Medicine, as well as co-director of the Division of Infectious Diseases. She, likewise, holds the Theodore and Bertha Bryan Professorship in Environmental Medicine. Her laboratory is examining another aspect of the immune system. TB is clever, but by bolstering our defenses, we may prevent drug resistance and reduce treatment duration. “If it required two weeks rather than six months to treat TB,” Philips states, “that would alter the course of the epidemic.”

Currently, Philips is concentrating on the relationship between TB’s lipids and macrophages in the immune system, another type of cell that is intended to eliminate and eradicate bacteria but falters with TB. Several varieties of macrophages exist, and TB possesses distinct strategies to counter each one. What is the most effective way to retaliate?
She is also investigating the immune system’s T cells, which assist in rendering macrophages lethal to intruders. How can we fortify that interaction? Moreover, she is exploring cholesterol, which TB siphons from its host for sustenance. “TB alters cholesterol,” Philips mentions, “in a manner that our body does not. We believe it does this to modify the immune reaction. We aim to comprehend that mechanism.” Furthermore, because these modifications could be identified in the blood, they may provide a novel approach to diagnose TB. A blood test could be simpler and potentially more informative than a sputum sample. The easier we make diagnosis and treatment, the more effectively we can manage TB’s transmission.
The hurdles to public health
The diagnosis of TB and management of its spread fall under the responsibility of Thomas Bailey, MD, a professor of medicine at WashU and medical director of the General Infectious Diseases Clinic, as well as the medical director of the TB prevention program for the St. Louis County Department of Public Health. When a WashU Medicine physician at Barnes-Jewish Hospital has concerns that a patient may have TB, Bailey is consulted. When an individual arrives at the county health department with symptoms, Bailey collects sputum samples and receives the results of a molecular test within a day or two, identifying not only the infection’s presence but also any mutation in the TB gene that indicates antibiotic resistance.
“Many of these individuals have already consulted multiple doctors,” he explains, “because TB is so rare here that it’s possible to complete medical education without encountering a case.” This complicates diagnosis — particularly with TB occurring outside the lungs, as happens in 15% of cases.
“You inhale it, the organism multiplies, and before the immune system can halt it, it has spread throughout your body — in a process that’s entirely without symptoms,” Bailey elucidates. A patient’s chest X-ray may appear entirely normal, as the TB there might have resolved, yet it could have advanced to the brain or bones.
It is challenging to communicate a sense of urgency, Bailey mentions, since TB is infrequent in the U.S.: “about 10,000 individuals each year, contrasted with a global incidence that’s nearly 11 million. Furthermore, approximately three-fourths of TB patients in the U.S. were born outside the nation.”

However, there are additional risk factors. TB has surged globally since the pandemic. Both the SARS-CoV-2 virus and the medications utilized against it led to immune system suppression, rendering people more vulnerable to TB. Simultaneously, the healthcare system was inundated, diverting public health resources from TB management to confront COVID-19. Additionally, people were hesitant to seek treatment for a minor chronic cough. Or severe night sweats. Or, as time progressed, the blood they began to cough up.
Since the pandemic, TB cases have escalated by at least 7% annually — coincidentally, at the same rate they previously declined. In 2023, the U.S. reported 9,600 cases; by 2024, this number had increased to 10,300. The highest rates are found in populous states such as California, Texas, New York, and Florida; Missouri has a low incidence, with only 74 cases in 2023 and 85 in 2024. It was thus shocking when the number of cases in Kansas rose from 46 in 2023 to 115 in 2024, marking a 150% increase.
The Kansas outbreak, with
“““html
Cases of clustering in Kansas City appeared to be an outlier — yet there will be increasingly more outliers.
“If we ever aim to eradicate TB, and this conversation continues, we will require a suitable vaccine.”
Thomas Bailey, MD
“If we ever aim to eradicate TB,” Bailey states, “and this conversation persists, we will require a suitable vaccine.” He exhales slowly. “It demanded significant financial resources and effort to regain control over TB in the ’90s. The standard approach became directly observed therapy, which is resource-heavy.” After studies indicated that only around 11% of patients completed the six-month treatment, health department personnel have been closely monitoring patients as they take their medicine. (Now, there’s a secure app where patients can videorecord their dosages.)
From 2003 to 2016, to conserve funds and enhance adherence, public health specialists attempted to reduce the duration of therapies and even proposed that administering antibiotics two to three times weekly might be effective. “It took many years,” Bailey remarks solemnly, “to realize that the relapse rate was unacceptably high.”
Not only does TB’s treatment regimen require extended duration, but culturing a sputum specimen can also take up to eight weeks. Allison Eberly, PhD, is an assistant professor of pathology and immunology at WashU Medicine and one of the medical directors at the clinical microbiology lab.
Over the past ten years, molecular testing has made a significant impact, but she still monitors cultures for as long as 56 days, “because no test is flawless.” She also has to send samples to a public health laboratory due to their advanced molecular techniques and sequencing capabilities that can identify antimicrobial resistance.
What she discovers about ten times more frequently than TB, however, are the other mycobacterial infections that Stallings alluded to. A molecular test for those infections is urgently needed, so patients can gain a quicker diagnosis.
Since non-TB mycobacterial infections are not reportable illnesses in many regions, tracking the infection rate is challenging. Nevertheless, akin to TB, the majority of these infections necessitate a regimen of three to four drugs and may take months or years to treat.
The stigma of contagion
Individuals with TB not only dislike the six-month antibiotic regimen and its side effects, but they also hesitate to disclose their condition. Why does stigma persist in this modern era? Because it is frightening, transmissible, and chronic. Because it can linger in the body indefinitely, and the treatment—at least in the U.S.—is intrusive, with health department personnel arriving like Mary Poppins to watch them take their medication. Furthermore, the 19th-century allure is gone: TB is now viewed as a disease affecting the impoverished.
The group most vulnerable to TB, of course, includes individuals with weakened immune systems. They might be undergoing treatment for rheumatoid arthritis or another autoimmune condition, or they may be HIV-positive, elderly, underweight, smokers, diabetics, individuals with head, neck, or gastric cancer, organ transplant recipients, or those with kidney failure. However, the most prevalent risk factors are the familiar foes of health: malnutrition; overcrowding; homelessness; substance misuse; and limited accessibility to, or distrust in, healthcare. “TB is both a manifestation and a reflection of injustice,” writes John Green in his poignant and thorough New York Times bestseller, Everything Is Tuberculosis.
“TB is predominantly a disease found in low-income nations. And we inhabit a world that overlooks those with fewer resources and diminished power.”
Sandro Galea, MD, DrPH
The dean of the new WashU School of Public Health, Sandro Galea, MD, DrPH, views TB as a crucial disease that students ought to study as part of a holistic public health education. Topics such as raising awareness, combating stigma, enhancing diagnosis and treatment access, encouraging patients to complete their therapy, and addressing the fundamental social forces that place individuals at risk are essential for public health and crucial for all students to comprehend.
“TB is predominantly a disease found in low-income nations,” Galea articulates. “And we inhabit a world that overlooks those with fewer resources and diminished power.” He adds that we also exist in an environment where “TB will not honor borders. It will expand.” Travel constitutes a risk factor, particularly to regions where TB is prevalent, which includes areas of China and India, the rest of South and Southeast Asia, Africa, Eastern Europe, the Caribbean, Latin America, the Middle East, and the Pacific Islands.
The funding dilemma
Prior to the federal government’s cuts to USAID, the global response to TB was already approximately $11 billion lacking in the financial support needed to manage the infection, according to Stallings. Now, USAID is unable to provide antibiotics for TB treatment, which leads to more fatalities and increased contagion — followed by even more deaths and further contagion. Shipments of antivirals for AIDS have also been halted, resulting in even greater vulnerability to TB, as an immune system requires the T cells being compromised by AIDS to combat TB.
“My entire lab operates on federal funding,” Stallings indicates, her tone tense. “We’ve already experienced delays on a couple of grants initially set to commence on March 1, aimed at developing new antibiotics. We collaborate with Fimbrion Therapeutics (whose chief scientific officer Thomas Hannan, DVM, PhD ’08, is a WashU alumnus) to transform our laboratory findings into treatments. Fimbrion has been developing these drugs, and they are performing excellently. The grant would facilitate their entry into clinical trials — but funding is currently stalled.”
Bailey can already anticipate the arguments for reductions: “‘It’s merely 10,000 people annually; why do we need such extensive funding to care for them?’ Believe me, it’s not to fund inflated salaries for healthcare workers,” he emphasizes. “The individuals I work with at the health department are nearly saintly. They treat patients with the dignity they deserve while earning very little. Some hold multiple jobs.” Public health expenditures could be efficiently lowered if we had an effective vaccine, yet significant federal grants allocated for vaccine development at other institutions are slated to be reduced.
By investing in foundational research, drug development, and public health, the U.S. has successfully controlled a disease that runs rampant in many other parts of the world, Bailey underscores. Once TB spreads that extensively, even the most robust public health initiatives become overwhelmed. “A nation like India has so many cases that it cannot hope to maintain TB control, especially without an effective vaccine.”
“When public health is underfunded, illnesses surge … and that’s exactly the trajectory we are heading towards now.”
Sandro Galea
Galea once co-authored a study assessing the repercussions of reduced public health financing after New York City’s 1975 fiscal crisis and the Reagan-era federal budget cuts. The results were published in the American Journal of Public Health, and the accompanying graph depicts the narrative: the TB incidence rate dramatically increased following the cuts, resembling a mountain that peaks in 1993 before finally tapering off. HIV and other public health threats also escalated after the cuts. Overall, the downsized budget initially saved New York City $10 billion — but ultimately cost the city more than $50 billion.
“When public health is underfunded, illnesses surge,” Galea states today. “New York witnessed a massive outbreak, and that’s precisely where we are headed now.”
The conclusion
In the last five to ten years, “we have acquired so much knowledge about TB infection progression, its pathogenesis, and its disease mechanisms,” notes WashU Medicine’s Philips. Now, she emphasizes, we require an effective vaccine. We need additional strategies and therapies that can incapacitate TB, outsmart multidrug-resistant TB, and bolster and redirect the immune response. We must also comprehend what reactivates latent TB. Moreover, we need to enhance public awareness regarding the deadliest disease worldwide.
“With USAID initiatives halted, we will see the numbers rise — and that will inevitably spread to this country.”
Jennifer Philips, MD, PhD
“If fortune favors us,” Bailey states, “and scientific exploration continues unimpeded, without entirely eroding public confidence in vaccines” — we may maintain control, at least within this nation. “But TB is a disease highly adapted to humans. If we divert our attention …”
Stallings shares his concern. “TB has evolved alongside us — and it adapts more swiftly than we do. We must find ways to stay ahead.”
If we fail? “With USAID efforts shuttered, we will witness a continual rise in numbers — which will inevitably spread here,” Philips warns.
Already, the fatality rate is escalating, Galea adds. “We could certainly witness a resurgence of TB in this country.”
The post The world’s deadliest disease appeared first on The Source.
“`