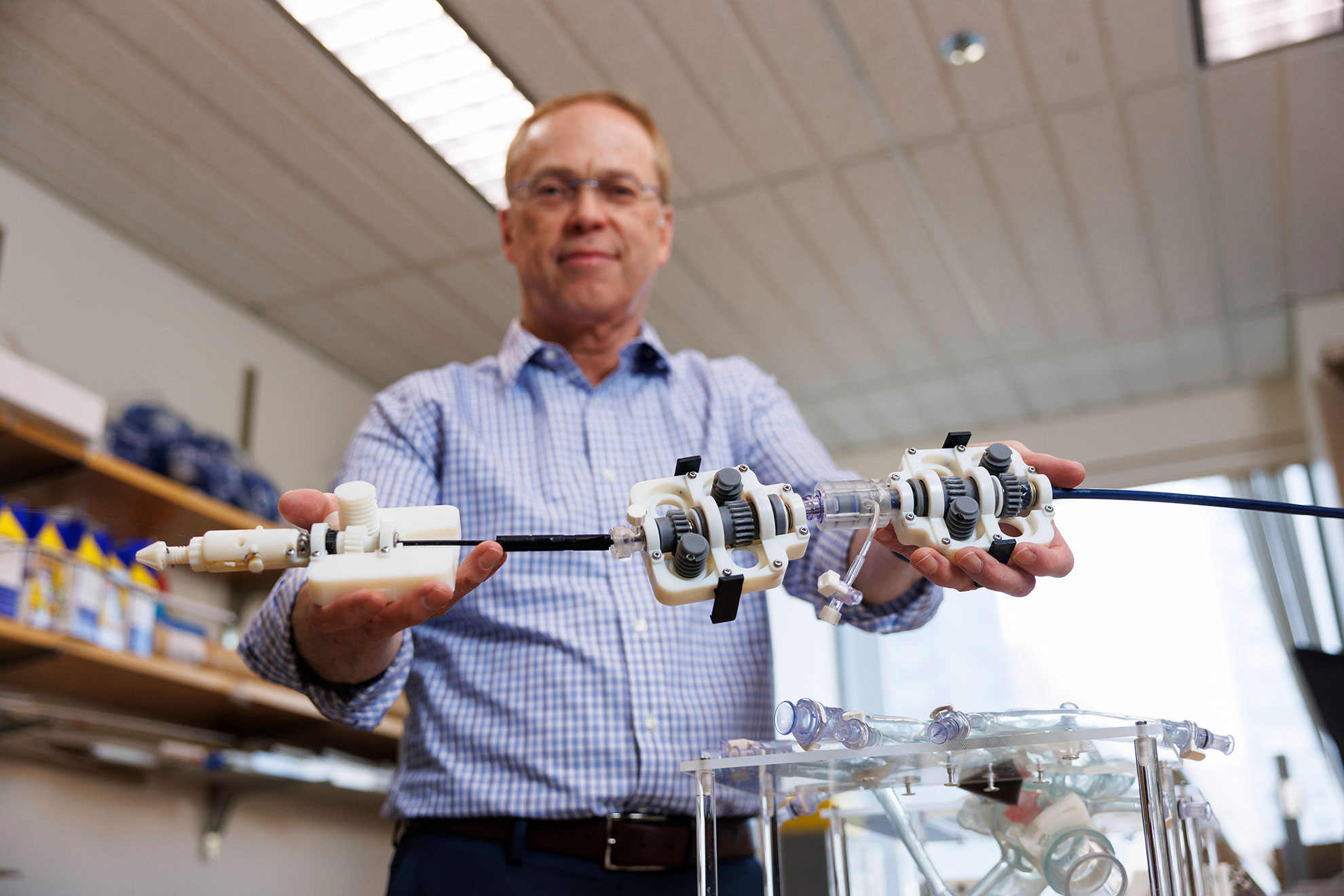
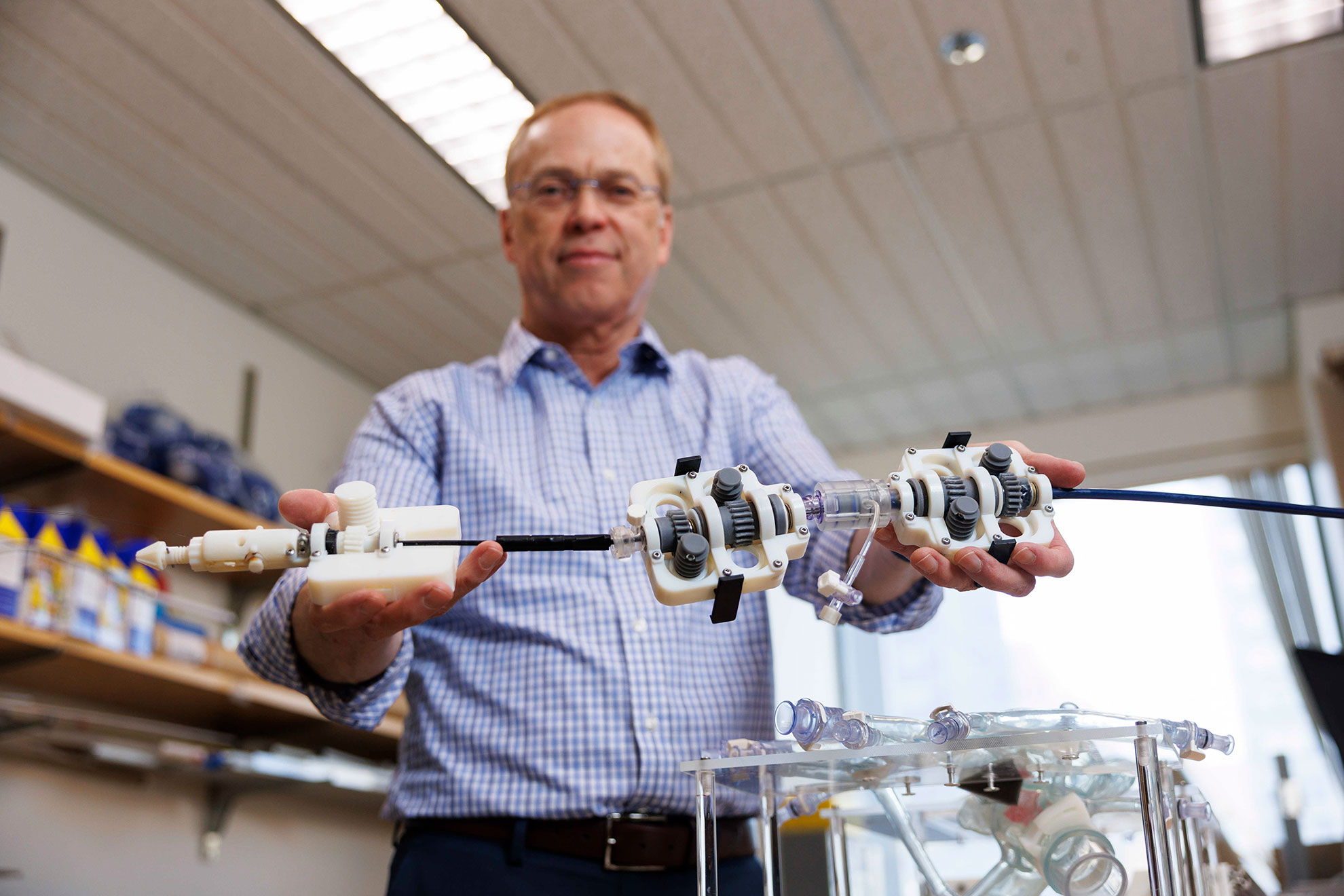
Pierre E. Dupont showcases a transcatheter valve repair device equipped with a motorized catheter drive system, superseding the conventional manual handle.
Niles Singer/Harvard Staff Photographer
Alvin Powell
Harvard Staff Writer
8 min read
Expert in medical robotics asserts that forthcoming autonomous devices will enhance clinicians’ abilities (not replace them), broadening access to advanced procedures
The robotic physician will assist you now? Not in the near future, at least.
Contemporary medical robots are rather limited, generally functioning as extensions of a surgeon’s hands instead of substituting for them. Pierre E. Dupont, a surgical professor at Harvard Medical School, co-wrote a Viewpoint article in Science Robotics last month, indicating that autonomous surgical robots that adapt and learn are on the horizon.
Nonetheless, their anticipated effect will be to enhance clinicians’ skills rather than replace them, and to expand the reach of pioneering techniques beyond the urban settings of academic medical institutions where they usually arise.
In this adjusted dialogue, Dupont, who also leads pediatric cardiac bioengineering at Boston Children’s Hospital, conversed with the Gazette about the areas most likely to see surgical robots functioning autonomously, and some obstacles to their implementation.
You point out that technologies for robot autonomy and learning systems are being applied in both manufacturing and medical environments. How does that function?
Indeed, in nearly every other sector, robots are utilized as independent agents to replace the labor that would normally be needed for a task. However, in various surgical fields, such as laparoscopy, they serve as extensions of the surgeon’s hand. They improve ergonomics for the surgeon, but questions remain about how significantly they enhance the patient’s experience.
Outside of healthcare, teleoperation, where the operator employs a mechanical input device to directly control the robot’s movement, is only implemented in remote or hostile environments like outer space or the ocean floor. Yet, this is how laparoscopic robots are operated.
A current exciting development, which ties into hospital economics, is telesurgery, where a hospital based in Boston connects with satellite facilities in suburban areas. Instead of the surgeon being present with the patient in the operating room, robots would be stationed at these satellite locations, allowing the surgeon to remain at the primary hospital and connect remotely to carry out procedures. This is trending today, albeit not automated.
What would an automated procedure entail?
Some simpler medical procedures are already automated using non-learning methodologies.
For instance, in joint replacement, a cavity must be formed in the bone to insert an implant. Historically, the surgeon’s expertise dictated how well the implant aligned and whether the joint was properly aligned.
There is a strong alignment with machining processes, which motivated the invention of robots to mill cavities in the bone — achieving more precise and consistent results. This has become a significant market within orthopedics.
The autonomy of the milling robot exists because it presents a well-structured problem and is straightforward to model. A 3D representation of the bones is created, and the surgeon can sit at a computer interface, utilizing software to define precisely how the implant will align and how much bone will be extracted. Everything can be modeled and preplanned — the robot simply executes the plan. It’s a rudimentary form of automation.
“Instead of the clinician being with the patient in the operating room, you would have robots at the satellite hospitals, and the clinician could stay at the main hospital and connect remotely to perform procedures.”
Pierre E. Dupont
This is due to the characteristics of the bone and the implant. The measurements are predetermined. Nothing shifts as it would if you were operating on a beating heart.
Correct, although I believe transcatheter cardiac procedures and general endovascular processes are actually excellent candidates for automation.
The geometry is less clearly defined than in orthopedic surgeries, yet it is still much more straightforward than in laparoscopy or any open surgery involving soft tissue.
In soft tissue surgeries, forceps, scalpels, and sutures are utilized to grasp, cut, and stitch tissue. The clinician, through experience, holds a mental model of how firmly they can grip the tissue without harming it, how it will deform when they pull and cut, and how deep they must insert the needle while suturing.
These variables are much harder to model using traditional engineering techniques compared to milling bone.
To what degree is the advancement in this domain attributed to the speed of technological growth versus acceptance among clinicians and patients?
If one solely considers robotics, the level of acceptance is quite surprising. Many academic clinicians enjoy experimenting with new technologies. Numerous patients, perhaps mistakenly, presume that the clinician must perform better with this remarkable equipment.
Hospitals prioritize financial implications. They don’t necessarily care if the clinician’s back is slightly less fatigued at the end of the day due to robot usage. They want to know whether the patient experiences fewer complications and is discharged sooner — in other words, improved care for reduced costs. That’s the challenging aspect: Robots generally require more investment for development and deployment compared to most other medical devices.
“““html
When discussing the acceptance of automation in medical robotics, healthcare professionals may express some hesitation as they ponder if they might be replaced. However, it’s more akin to providing them with a powerful instrument that can enhance their expertise.
Numerous practitioners may encounter a specific procedure merely ten times annually. Consider any complex task in life that you perform monthly; you wouldn’t execute it with the same proficiency or confidence as if you were doing it daily.
Therefore, if the robot isn’t supplanting them but functioning as a highly skilled partner with whom they can interact, offering guidance through the procedure — stating, “Now I’ll proceed with this.” Or querying, “Do you believe this is the correct approach?” or “Should I place this device slightly to the left?” I anticipate a positive reception. Should a system facilitate a clinician’s learning curve and rapidly enhance their skill level, every clinician would desire one.
How significant are recent developments in large language models and alternative AI forms in the realm of autonomy?
These advancements are set to drive innovations in medical robotic autonomy. We are developing transcatheter valve repair techniques that are currently performed manually. Clinicians must execute numerous procedures to become proficient — and maintain that proficiency.
Our research has demonstrated that incorporating robotic teleoperation simplifies these tasks. By integrating learning-based autonomous capabilities, we could ensure these procedures are safely performed in lower-volume facilities.
This is crucial since a primary concern is accessing top-tier care and the latest treatments primarily available in major urban centers housing academic medical institutions. However, many individuals do not reside in those regions and prefer to receive treatment locally, even if travel is an option.
Thus, empowering community hospitals to provide these services, albeit at lower volumes, offers an opportunity for a significantly larger segment of the population to access leading medical care.
Looking ahead, do you have any reservations about the increasing autonomy in medicine?
I see considerable potential for advancing levels of autonomy, but it must be implemented incrementally. Patient safety must always remain a priority in the regulatory process.
There will inevitably be unforeseen occurrences, such as atypical anatomical structures, that the system hasn’t been conditioned to handle. It’s essential that the system has the ability to identify these challenges as they arise — it must recognize when it is outside its limits.
Currently, this represents an area of study in learning systems — there’s still technology to be developed. Nevertheless, the progress observed in foundational models over the past few years has illustrated the potential that exists.
Ultimately, will there be a scenario with no clinician involved? That question can be postponed for now.
You mentioned that these systems come with a high price tag. Will costs decrease as they become more prevalent?
The obstacle is that medical devices are tailored and authorized for specific applications. To develop a new medical device, one must assess how many procedures are carried out annually, as well as the reimbursements linked to those procedures.
For any medical device — excluding robots — the smallest viable market size is $100 million in sales each year. And for attracting venture capital, the market should ideally be at least a billion dollars.
Given the substantial development costs of medical robots, this implies the need for a multi-billion-dollar market for such devices. Existing markets do exist: Laparoscopy and orthopedics presently serve as examples. Endovascular procedures, including heart valve repair and replacement, are another target area for me.
A crucial factor for each of these three instances is that the robot functions as a platform. It can be applied to various procedures, thus presenting a much broader addressable market compared to a robot limited to a singular task.
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.